
No Scalpel Vasectomy

Pre-Vasectomy Counseling
Vasectomy is a safe and effective method of birth control. This operation is only carried out when you are certain that you have fathered all the children you wish to have. Vasectomy should be viewed as a permanent form of contraception with only a possibility of reversibility.
It important to take time for reflection before electing to undergo vasectomy and reconsider alternative contraceptive methods. Preoperative sperm-banking and post-operative vasectomy reversal and sperm retrieval (for subsequent in vitro fertilization) can be discussed if you are concerned about the permanent nature of the procedure.
No-Scalpel Vasectomy
Vasectomies are usually performed in the office. In the procedure room, the scrotal anatomy will be washed with an antiseptic solution. Local anesthesia will be injected to numb the area, but you'll be aware of touch, tension and movement.
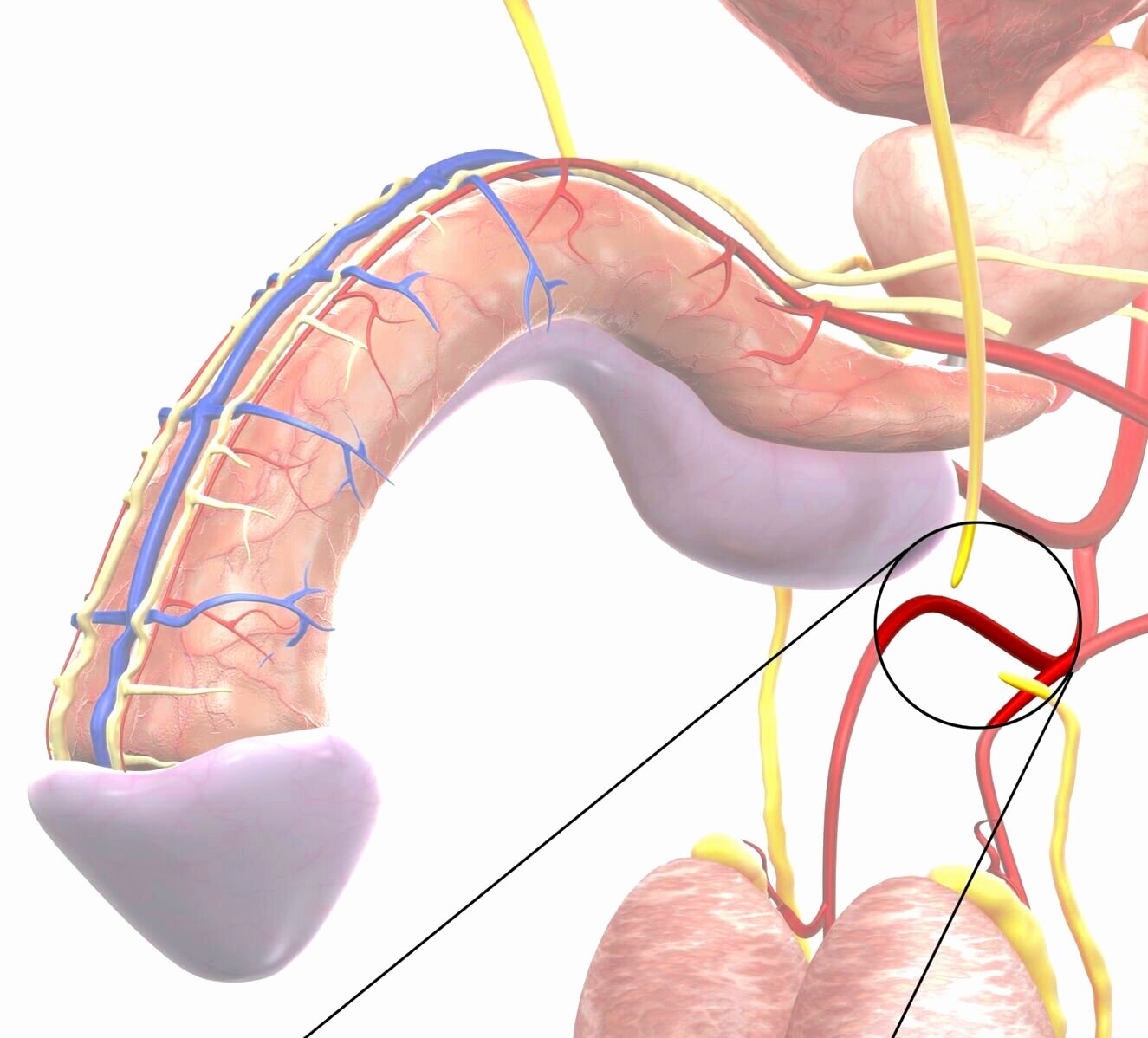
During the procedure, the vas is palpated under the skin of the scrotum and is held in place with a small clamp.
A tiny hole is made in the skin and stretched open so the vas deferens can be gently lifted out.
It is then cut, tied or seared and put back in place.
What are the Risks of Vasectomy?
Common – greater than 1 in 10
Bruising and swelling of scrotum/penis for several days
The wound may be weepy
Seepage of a small amount of clear, yellow fluid several days later
Blood in semen for the first few ejaculations
Occasional – approximately 1 in 50
Significant bleeding or bruising requiring further surgery
Inflammation or infection of the testes, epididymis or wound needing antibiotics
Chronic testicular pain
Pain during intercourse
Rare – less than 1 in 50
Early or late failure
Rejoining of the ends of the vas, after negative sperm counts, resulting in fertility and pregnancy at a later stage
The early failure rate of vasectomy (presence of motile sperm in the ejaculate at 3–6 months post-vasectomy) is in the range of 0.3–9% and the late failure rate is in the range of 0.04–0.08%.
Granuloma – lump of tissue that can be felt
Hydrocele
Frequently Asked Questions
Can my partner tell if I have had a vasectomy?
Sperm adds very little to the semen volume, so you shouldn't notice any change in your ejaculate after vasectomy. Your partner may sometimes be able to feel the vasectomy site. This is particularly true if you have developed a granuloma.
Will my sense of orgasm be changed by having a vasectomy?
Ejaculation and orgasm are usually not affected by vasectomy. The special case is the rare man who has developed post-vasectomy pain syndrome.
Can I become impotent after a vasectomy?
An uncomplicated vasectomy can't cause impotence.
Can a vasectomy fail?
There is a small chance that a vasectomy may fail. This occurs when sperm leaking from one end of the cut vas deferens finds a channel to the other cut end.
Can something happen to my testicles?
In rare cases, the testicular artery may be hurt during vasectomy. Other problems, such as a mass of blood (hematoma) or infection, may also affect the testicles.
Can I have children after my vasectomy?
Yes, but if you haven't stored frozen sperm you'll need an additional procedure. The vas deferens can be microsurgically reconnected in a procedure called vasectomy reversal. If you do not want to have vasectomy reversal, sperm can be taken from the testicle or the epididymis and used for in vitro fertilization.
These procedures are costly and may not be covered by your health plan. Also, they don't always work. If you think you may want to have children one day, you should look into nonsurgical forms of birth control before deciding to have a vasectomy.